22Y/O FEMALE WITH DRUG INDUCED RASH
This is an online E-log entry blog to discuss and understand the clinical data analysis of a patient, to develop competency in comprehending clinical problems, and providing evidence- based inputs in order to come up with a diagnosis and effective treatment plan to the best of my ability.
A 22 year old female,R/O Nakrekal, who is a Student,came with the chief complaints of
1)Itching all over body since 5 days.
2)Rashes all over body since 5 days.
History of presenting illness:
The patient was apparently asymptomatic
1month back when she developed rashes
over arms,legs and abdomen after contact
with some plants in her lemon field for
which she went to a local doctor for
treatment,where she was prescribed steroid
ointment(halobetasol proprionate) and oral
medications,which she took for 10days and
the rash subsided but blackish spots
remained over skin.
10 days back(21-10-21) she developed fever which was high grade , intermittent associated with chills,vomitings and generalised body pains,fever decreased on taking medication.
Vomitings since 10 days ,4-5 episodes per day,food particles were the contents,non bilious,non projectile associated with nausea.
She went to local RMP for fever and vomitings , where she was diagnosed with typhoid associated with jaundice. They gave her IV saline and paracetamol.
The next day (6 days ago,24-10-21),they went to a ayurvedic doctor for jaundice where she was prescribed a herbal medication. She took the medication on that day.
Next morning (5days ago,25-10-21),she was having itching and burning sensation and rash all over her body. The rash were of variable size,non blanchable all over her body i.e limbs,chest,abdomen,back and groins.
She went to Nakrekal hospital on same day where she was given soap and lotion.
Because symptoms were not relieved, she went to Suryapet hospital next day where she was prescribed doxycycline,sucralfate and lotionafter which the itching decreased but erythema and rashes remained.
The next day (3 days ago 28-10-21)she developed edema in her arms first and then generalised edema. She was brought to our hospital.
No h/o cold,cough and abd pain.
Past History:
One month ago h/o rash after contact with something in her lemon field for which she took steroids.
No h/o DM,HTN, Asthma,TB, Epilepsy.
Personal History:
Diet: Mixed.
Appetite: Normal.
Sleep: adequate.
Bowel movements: hard stools passed once in 2 days.
Bladder movements: Regular.
No addictions.
Treatment History:
No known drug allergies.
Steroids one month back for 10 days
She took saline and paracetamol 8 days back.
Herbal medication 6 days back.
Saline, soap, lotion 5 days back.
Doxycycline, sucralfate, lotion 4 days back.
Family History:
Insignificant.
General Examination:
Patient was examined in a well lit room with informed consent.
She was conscious, coherent, co-operative; well oriented to time, person and place.
Moderately built, well nourished.
Pallor: absent
Icterus: present
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Edema: present
Vitals:
TEMP- 101°F
PULSE- 120 bpm
RR- 20 cpm
BP- 90/70 mmHg
SPO2- 99@ROOM AIR
GRBS- 86 mg/dl.








Systemic Examination:
CVS: S1, S2 heard, no murmurs
Respiratory: BAE positive, NVBS heard
P/A: Soft, nontender
CNS: No abnormalities detected
Cutaneous examination: Diffuse erythematous non-blanchable purpura of variable size noted all over body. Facial edema noted. No oral or genital mucosal involvement.
INVESTIGATION:
1)HAEMOGRAM.

2)COMPLETE URINE EXAMINATION:

3) BLOOD GROUPING AND RH TYPING:

4)PT:

5)APTT:

6)LIVER FUNCTION TESTS: RAISED LFT'S EXCEPT A:G RATIO.

7)RENAL FUNCTION TESTS:



8)RANDOM BLOOD SUGAR:

9)RAPID DENGUE TEST:

10)ECG
11)USG ABDOMEN:
-GALLBLADDER EDEMA,
-MILD SPLENOMEGALY
-MINIMAL ASCITES.
12)2 D ECHO.

DVL REFERRAL DONE:
O/E: DIFFUSE ERYTHEMATOUS (NON BLANCHABLE) PURPURA OF VARIABLE SIZE ARE NOTED OVER THE BODY i.e,BOTH UPPERLIMBS,LOWER LIMBS,CHEST, ABDOMEN,BACK &GROINS
EDEMA IS NOTED(FACIAL)
NO ORAL , GENITAL MUCOSAL INVOLVEMENT.
DIAGNOSIS:DRUG RASH -(DRESS SYNDROME)
TREATMENT SUGGESTED:
1.STOP THE OFFENDING DRUG
2.TAB.ATARAX 25MG OD x 2WEEKS
3.VENUSIA MAX LOTION L/A BD x 2WEEKS


TREATMENT GIVEN HERE :(29/10/2021)
1.T.UDILIV 300mg PO/BD
2.SYRUP. LACTULOSE 15ml PO/OD IN NIGHT
3.T.ATARAX 25mg PO/OD IN NIGHT
4.T.PCM 500mg PO/SOS
5.T.RIBOFLAVIN 10MG PO/BD.
DAY-2:(30/10/2021)
Soap notes
S:
Itching decreased
Rashes present
O:
PR: 92bpm
Bp: 110/80mmhg
Temp: 98.5F
RR:18cpm
Cvs:s1,s2heard
Rs:BAE+
CNS:NFD
Generalised edema present.
Rashes present all over the body
A:
Hepatitis secondary to Drug induced(herbal medication)
INVESTIGATIONS ON DAY2(30/10/2021):
1)HEMOGRAM.

2)RETICULOCYTE COUNT:

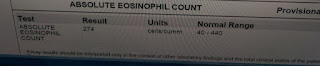
3)ABSOLUTE EOSINOPHIL COUNT:
4)LFT

5)LDH:

6)CRP -POSITIVE

7)COOMBS -POSITIVE.
P:
1)Tab.UDILIV 300mg PO/BD
2)SYP.Lactulose 1ml/po/H/s
3)Tab.ATARAX 25mg PO/OD/Hs
4)Tab.RIBOFLAVIN 10MG PO/BD
DAY-3:(31/102021)
Soap notes
Icu 6th bed:
S:
1 Fever spike at 4:00am
Itching decreased
Rashes present
O:
PR: 82bpm
Bp: 120/80mmhg
Temp: 99F
RR:18cpm
Cvs:s1,s2heard
Rs:BAE+
CNS:NFD
Generalised edema present.
Rashes present all over the body
A:
Hepatitis secondary to Drug induced(herbal medication)
Investigations on day3(31/10/2021)
1)HEMOGRAM:

2) LFT:

3)S.CREATININE:0.4mg/dl
P:
1)Tab.UDILIV 300mg PO/BD
2)SYP.Lactulose 15ml/po/H/s
3)Tab.ATARAX 25mg PO/OD/Hs
4)Tab.RIBOFLAVIN 10MG PO/BD
5)Tab.PCM 500mg PO/SOS
6)Tab.Zincovit po/od.

DAY-4:(01/11/2021)
Icu 6th bed:
S:
Continuous fever spikes present whole night
Itching decreased
Rashes present
O:
PR: 120bpm
Bp: 120/80mmhg
Temp: 98.1F@ 7am
RR:18cpm
Cvs:s1,s2heard
Rs:BAE+
CNS:NFD
Generalised edema present.
Rashes present all over the body
A:
Hepatitis secondary to Drug induced(herbal medication)
P:
1)Syp.LACTULOSE 15ml/po/H/s
2)Tab.ATARAX 25mg PO/OD/Hs
3)Tab.RIBOFLAVIN 10MG PO/BD
4)Tab.PCM 500mg PO/SOS
5)Tab.ZINCOVIT po/od
6)Inj.CEFTRIAXONE 1gm/iv/bd(D1)
DVL review done:
O/E: MULTIPLE,VIOLACEOUS,HYPERPIGMENTED PLAQUES AND PAPULES(NON TENDER) NOTED OVER ALL THE FOUR EXTREMITIES, ABDOMEN.
SCALY PLAQUES NOTED OVER THE GROIN(BOTH)
ORAL MUCOSA -PIGMENTATION(BUCCAL MUCOSA).


DIAGNOSIS:
?LICHEN PLANUS
?LICHENOID DRUG ERUPTION+DRUG RASH
ADVICE:
-CRP
-SKIN BIOPSY
TREATMENT SUGGESTED:
1.STOP THE OFFENDING DRUG
2.VENUSIA MAX LOTION
3.Tab.ATARAX 25mg sos.

DAY-5(02/11/2021):
Soap notes
S:
Fever spikes present
Itching has decreased
Rashes present
O:
PR: 88bpm
Bp: 120/80mmhg
Temp: 103.5F @ 8am
RR:24cpm
Cvs: S1,S2 heard
Rs: BAE+
CNS:NFD
Pallor+,Icterus+.
Generalised edema present.
Rashes present all over the body
A:
Hepatitis secondary to Drug induced(herbal medication)
Haemolytic anaemia
with ?lichen planus ? DRESS syndrome
Investigations on day5(02/11/2021)
1)HEMOGRAM:

2)LFT:

3)RFT:



P:
1)Syp.LACTULOSE 15ml/po/H/s to maintain 2 episodes of loose stools
2)Tab.ATARAX 25mg PO/OD/Hs
3)Tab.RIBOFLAVIN 10MG PO/BD
4)Tab.PCM 500mg PO/SOS
5)Tab.ZINCOVIT po/od
6)Inj.CEFTRIAXONE 1gm/iv /bd *day 2
7)Tab.UDILIV 300mg/BD
7)LULIFIN cream L/A BD
8) plan to start oral steroids if there is further drop in haemoglobin.



Comments
Post a Comment